





BCC skin cancer
BCC skin cancer - Skinsite's digital imaging picks up the small red lines
BCC skin cancer - other digital imaging can miss the red lines
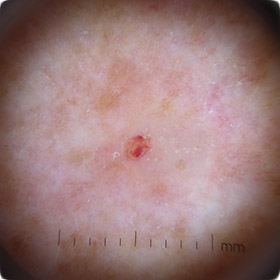
Nodular BCC
BCC skin cancer
BCC skin cancer
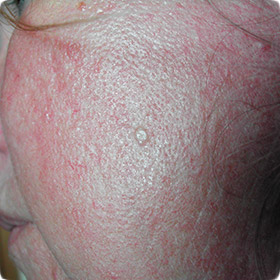
Superficial BCC
BCC skin cancer
Basal Cell Carcinoma (BCC)
BCC Skin Cancer
It is estimated that over 50,000 non-melanoma skin cancers develop in New Zealand each year and the most common of these is basal cell carcinoma (BCC). Fortunately this is the least dangerous of the skin cancers but the risk is with local spread and destruction of tissues.
BCC is a cancer of the cells at the base of the epidermis. Intermittent UV exposure is a major causative factor and lesions will often appear in parts of the body which are kept shaded. These include the areas around the nose, in the temples, around the eyes, on the neck, back and upper limbs.
Nodular BCC will present initially as a small glistening translucent or pearly lump that slowly enlarges. It may ulcerate and bleed and patients will report that it is a spot that doesn’t heal. Invariably there is no pain. It may ulcerate centrally, leaving rolled edges giving rise to the term ‘rodent ulcer’.
Superficial BCC presents as a red scaling patch and most commonly occurs on the trunk. It can be mistaken for an area of eczema.
Whilst basal cell carcinomas do not spread they can grow relentlessly and destroy local tissue, eating into bone and cartilage. The morphoeic subtype is most dangerous in this regard as it can have root like projections which are difficult to detect clinically.
At Skinsite we have found that early BCC detection is greatly assisted by the technique of dermoscopy. In particular with nodular BCC there are tiny veins which run across the tumour’s surface that have a ‘focused’ appearance, which is usually invisible to the naked eye.
The BCC treatment of choice is usually by surgical excision. Other modalities include radiotherapy, cryotherapy (liquid nitrogen), curettage and cautery, photo-dynamic therapy and topical chemotherapeutic or immune modifying agents such as imiquimod. Choice of treatment for BCC depends on a range of factors including BCC type, site, size and compliance of the patient.
An important point to remember is that once one BCC is diagnosed, the patient is at risk not only for further BCCs to occur, but also for SCC and melanoma to develop, hence the importance of regular skin cancer surveillance.